Wiskott-Aldrich Syndrome: Background, Pathophysiology, Epidemiology

Genetic Mutation
Genes are the inherited material you get from both your parents that are made from strands of molecules called DNA. Long stretches of DNA are packed with other materials, like proteins, to make 46 chromosomes. Genes contain the information, or "code", needed so your body can make the many proteins it needs to function. A genetic mutation is an alteration in the genetic code found in DNA.
A mutation changes the specific instructions of the gene, coded through small components of DNA. Because a genetic mutation changes the genetic coding, the resulting protein might not work the way it was initially supposed to, which can lead to disease.
Some mutations are present from birth. You can inherit some gene mutations that first occurred in one of your parents, grandparents, or an older ancestor. Other genetic mutations happen as a natural part of aging, and some happen after exposure to substances that cause damage to your DNA.
Design by Health / Getty Images
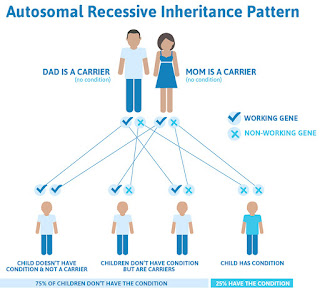
The types of genetic mutations are complicated because scientists conceptualize genetic mutations in different ways. They can be classified by the type of molecular genetic change, whether they're inherited vs. Acquired, or if they're dominant vs. Recessive. Type of Molecular Genetic Change Some mutations change just one tiny part of the genetic code, making it "incorrect." This might lead to a change in the effectiveness of the protein for which it codes. The protein might have missing parts, a part that doesn't work as well, a part in the wrong place, or it might not be made at all. Other types of mutations affect longer stretches of DNA and even more than one gene. For example, part of one gene might connect to the wrong part of the DNA sequence. This sometimes causes an abnormal combined protein to form. This kind of change can happen in some cancers. In some cases, large stretches of DNA are affected, and the mutation impacts multiple genes. Many genes might be completely absent, or there might be an extra copy of a long stretch of genes. One example is Down syndrome, in which the person has an extra copy of the genes found in chromosome 21. Not all mutations make a difference. Some "silent" mutations don't change how the protein functions, so they don't cause any problems. Inherited vs. Acquired Mutations You might inherit a mutated gene from one or both of your parents, meaning your parents had the mutation in their DNA and it became part of your DNA. In that case, you'd have the gene mutation in all your cells from conception. This might be important if the mutation directly causes a disease or greatly increases your risk of disease. A mutation like this might be passed down from generation to generation. The actual event that changed the DNA might have happened a very long time ago. In contrast, an acquired mutation occurs at some point later in life. It affects some of your cells, not all the cells in your body. It's normal to acquire new mutations as part of aging, and most of them don't make a difference. However, some acquired mutations can lead to cancer or other medical conditions. Scientists are still finding different types of gene mutations and determining how they are connected to certain diseases. Some related terminology is "germline" versus "somatic" mutation. A mutation in the germline affects the genes in the cells that one's children receive, so it can be transmitted across generations. However, mutations in other types of cells in the body, called "somatic cells," can't affect future generations. Dominant vs. Recessive Gene Mutations For some gene mutations that can cause disease, it matters whether you get a copy from just one or from both of your parents. Some diseases require you to have gene mutations from both of your parents in order for the disease to develop. Anyone can have a single gene mutation that doesn't cause illness; this is known as being a "carrier." For dominant gene mutations, having only one copy of the abnormal mutation can give you the disease. You can inherit it from either of your parent's DNA. For recessive gene mutations, you need to get copies of the mutation from both sides of your family to get the disease. Inheritance is also more complicated for mutations on the sex chromosomes (e.G., the "X" or "Y" chromosome). Depending on one's biological sex, you might need to inherit a gene from just one or from both parents to get the associated disease. You get inherited mutations from your parents. Even though the actual mutation occurred in your family's DNA long ago, scientists still refer to them as "mutations" if they result in certain diseases. Acquired mutations are caused by more recent changes to the DNA during one's lifetime. Getting some acquired mutations is a normal part of aging, but exposure to substances that can alter your DNA can increase your risk of getting more of them. Substances that increase the risk of such mutations can increase your risk of cancer. Examples include tobacco products, ultraviolet radiation from the sun, X-rays from medical imaging, radioactive substances (like radon), and many different chemicals. Scientists think that people inherit roughly 50,000 different genes, half from each parent. A genetic mutation can occur in any of these genes. The impact of a mutation varies widely based on the type of protein it affects and what that protein normally does. A mutation might affect your muscles, heart, digestive system, brain, blood, or any other body part. Because some proteins are expressed in more than one system, some mutations affect multiple areas. Some mutations are so severe that the fetus does not survive until birth. In cases of spontaneous miscarriage, at least half of fetuses carry a genetic mutation. These are typically severe chromosomal mutations involving many genes. Genetic Diseases vs. Multifactorial Diseases Some genetic mutations directly cause disease. For these kinds of diseases, sometimes called "genetic diseases," you need to inherit one (dominant) or two (recessive) copies of the abnormal mutation to get the disease. However, many diseases are multifactorial, meaning they have both genetic and environmental components causing them. Having variations of certain genes (i.E., having certain gene mutations) can increase your risk of a disease, but a lot more is involved. For example, having a certain gene mutation might slightly increase your risk of getting Alzheimer's disease. However, you wouldn't necessarily get Alzheimer's disease if you have this mutation, and some people without the mutation also get the disease. Harmful, Neutral, and Beneficial Mutations Most new mutations are neutral or harmful. However, some gene mutations cause advantageous protein changes. If so, that genetic mutation may eventually become widespread in the population. Mutations are a part of how species adapt to the environment over very long periods of time through the process of evolution. Thousands of different genetic disorders can affect human beings. Although they range from somewhat uncommon to exceedingly rare, together they affect around 1 in 12 people. Genetic diseases caused by inherited abnormal mutations include: Sickle cell disease (SCD): SCD causes a person's hemoglobin (a protein in red blood cells) not to form correctly, causing their red blood cells to form a "sickle" shape. It can cause anemia, repeated pain crises, and organ damage. Inherited thrombophilia: Sometimes called hereditary thrombophilia, this greatly increases your risk of abnormal blood clots that can affect the legs, lungs, or other parts of the body. A mutation in the prothrombin gene is a common cause of this condition. Hemophilia: This can cause frequent and severe bleeding. It is caused by mutations in genes such as FVIII which help make clotting factors to stop your body from bleeding. Familial hypercholesterolemia: Results from a genetic mutation can lead to very high levels of LDL-type cholesterol and can lead to heart attacks at a very young age. Cystic fibrosis (CF): CF is caused by mutations in the CFTR gene, which makes a protein responsible for the regulation of the chloride ion in cells. It leads to thick mucus build-up in the body, affecting the lungs, digestive tract, and other organs. Huntington's disease: Caused by mutations in the HD gene, this disease causes the nerves in the brain to break down. This can lead to involuntary movements and cognitive decline, among other symptoms. Duchenne muscular dystrophy: This condition generally affects males. It's caused by mutations in the DMD gene on the X chromosome and causes progressive muscle and skeletal weakness. Tay Sachs disease: This causes a build-up of fatty acids in the brain that progressively destroys cells in the nervous system. It results from a mutation on chromosome 15. Autosomal dominant polycystic kidney disease (ADPKD): Caused by mutations in the PKD1 or PKD2 gene, it causes abnormal cysts in the kidneys, which can cause kidney failure. Fragile X syndrome: This results from abnormalities in the FMR1 gene, leading to mental disability and other symptoms. Down syndrome: This causes mental disability and an increased risk of heart defects and digestive problems due to mutations leading to extra genes from chromosome 21. Cancer Acquired genetic mutations are part of what causes cancer. However, inheriting certain genes can increase your risk of developing these acquired mutations and, in turn, getting cancer. This is sometimes just a small increased risk, but the risk can be greater with some genes. For example, "BRCA" proteins are involved in DNA repair. Having a mutation in the BRCA1 or BRCA2 genes dramatically increases your risk of breast, ovarian, and some other cancers, and it increases your risk of getting these cancers at a younger age. Therefore, it sometimes makes sense to test for these mutations as part of preventive medical care, especially if you have a family member (such as your mother, aunt, or grandmother) who had breast or ovarian cancer. These tests are not part of routine preventative medical care. Individuals are selectively screened for risks and then tested based on their personal and family history. Genetic counseling is a good idea if you've been diagnosed with a genetic disease, have a known genetic disease in your family, or if you're displaying symptoms of a genetic disease. A specialist in genetics can talk to you about your risks of a certain condition in your specific medical context. Genetic testing is often needed to get a clear picture. To perform genetic testing, your healthcare provider will collect your DNA by swabbing your cheek or taking a sample of blood or saliva. Then your DNA will be examined in a laboratory to see if you have specific disease-causing mutations. Treatment for genetic mutations varies a great deal based on the mutation and the specific disease it causes. For example, treatment for muscular dystrophy varies quite a bit from treatment for a genetic problem that abnormally increases your cholesterol levels. Historically, healthcare providers haven't been able to directly treat the mutation itself. Instead, they focused on reducing symptoms and improving your day-to-day function. Depending on the situation, this might involve medications, changes in diet, and exercise, among other treatments and lifestyle factors. For acquired mutations leading to cancer, the focus is mostly on removing the unhealthy cells (e.G., through surgery, chemotherapy, or radiation). Newer technologies are making it possible to treat some genetic conditions at a deeper level. In a stem cell transplant, the approach is to wipe out your unhealthy blood-forming stem cells (containing the mutation). Then, you receive a stem donation from someone without the mutation, which eliminates disease symptoms. However, this isn't possible for all genetic conditions. Researchers have also developed gene therapies. These work by replacing or deactivating disease-causing mutations. This is a newer treatment area with potential risks, but it may eventually provide radically improved management for various genetic diseases, such as cystic fibrosis, hemophilia, and sickle cell disease. Although you can't always prevent getting a potentially harmful mutation or passing one on to your children, you may be able to reduce your risks. Preventing New Genetic Mutations in Yourself You can take steps to reduce your risk of getting potentially harmful mutations, including the following: Avoid tobacco products, all of which increase your risk of cancer and other disease Protect your skin from radiation from the sun by limiting exposure during the middle of the day and using sunscreen and coverups Eat a high-fiber diet with lots of fruits and vegetables Only get medical tests using radiation when truly needed, such as X-rays and especially CT scans Limit your consumption of alcohol Preventing Passing Down a Harmful Genetic Mutation In some diseases, parents can pass the disease to their children even if they don't have symptoms themselves. Genetic tests can show if you have a certain mutation that might cause disease in your child, so consult with an expert such as a genetic counselor. People who are carriers of disease-causing mutations have some options. For example, some people can use genetic testing paired with in vitro fertilization (IVF) to make sure their child won't have the disease mutation. You can also use genetic testing during pregnancy to see if a developing fetus carries specific gene mutations. Gene mutations can impact your health significantly. Depending on where they occur and their type, mutations can cause a broad range of disorders and diseases. When mutations occur in genes responsible for making important proteins, they can disrupt normal cell functions. Genetic mutations are classified in different ways, including the type of molecular genetic change, if they're inherited or acquired, or if they're dominant or recessive. Some genetic mutations directly cause disease while some require both genetic and environmental components in order to mutate. It is possible to develop thousands of genetic disorders, each very different from the last. You may be able to reduce your risk of developing a genetic disorder through some modifiable lifestyle factors. Genetic testing can also help your healthcare providers determine if you have certain gene mutations, if you're a carrier, or if your child is at risk of inheriting a mutation.Is Long Life Without Disease Possible? A Rare Genetic Syndrome May Point The Way
Ecuadorean doctor Jaime Guevara Aguirre, examines patients Maritza Valarezo (L) and her sister ... [+] Lugartda, both with Laron syndrome, during a consultation in Quito, on January 11, 2014. Physician and diabetes expert Jaime Guevara Aguirre, studies Laron syndrome, or Laron-type dwarfism, a disorder caused by a variant of the growth hormone receptor. The genetic mutation causes short stature and also prevents cancer and diabetes. AFP PHOTO / RODRIGO BUENDIA
AFP via Getty ImagesWe hear the words "genetic mutation" and tense up: if it's a mutation, it has to be a bad thing, right? Not always. In some cases, a mutation can offer protective or beneficial effects. These types of gene variants are a hotspot of research since they carry the promise of new treatments — if we understand how the mutation works, we may be able to mimic its protective effects artificially.
Laron syndrome, known technically as growth hormone receptor deficiency (GHRD), falls into this category. Individuals with the syndrome are much less likely to suffer from age-related diseases like cancer and diabetes. A new study suggests they may also be more resilient against heart attacks and other cardiovascular issues.
What is Laron Syndrome?Laron syndrome is an extremely rare disorder —there are less than 500 confirmed cases in the world— caused by mutations to the growth hormone receptor gene (GHR). As with any gene, the strand of DNA that comprises the growth hormone receptor is made up of thousands of "base pairs" — the chemicals that form the foundation of DNA. Just a single change to any of these base pairs may be enough to cause a difference in the function of the protein that the gene encodes.
These changes to the growth hormone receptor gene interfere with the production of important proteins involved in childhood growth. As a result, people with the syndrome are almost never taller than four and a half feet (1.5 meters). They are also prone to developing obesity and tend to have higher levels of low-density lipoprotein (LDL), or "bad cholesterol."
Despite this, people with Laron syndrome are long-lived compared to unaffected relatives. Back in 2011, a group of researchers suggested that this may be due to almost nonexistent levels of cancer and type two diabetes, lucky protective byproducts of the genetic mutation that causes the syndrome. Individuals with Laron syndrome tend to produce less of a growth hormone called insulin-like growth factor 1 (IGF-1), which although crucial for growth during childhood, has also been linked to the kind of haywire cellular proliferation that leads to cancerous tumors.
The same longevity boost has been observed in mice with Laron syndrome, who, compared to their peers, tend to live 40% longer. They also develop fewer tumors and exhibit the same smaller stature.
Another potential explanation for the increased lifespan of those with Laron syndrome is the fact that their cells are significantly more likely to self-destruct after suffering damage than those of unaffected individuals. This prevents the cells from accruing mutations or DNA damage over repeated generations, which is considered one of the hallmarks —and potential causes— of aging.
The same group of researchers, led by Dr. Jaime Guevara-Aguirre at the San Francisco de Quito University and Dr. Valter D. Longo at the University of Southern California, followed up these initial findings with a second study in 2017. This time, their research indicated that the protective effects of the syndrome were not restricted to the body alone: cognitive performance also remained high with age, and there were barely any cases of dementia. All in all, the brain function of older adults with Laron syndrome was closer to that of younger adults in the general population.
What About Heart Health?But one big question mark remained. Many researchers speculated that since those with the syndrome were more likely to develop obesity, they would also be more likely to develop heart issues. These issues could possibly outweigh the protective factors. To answer this question, Dr. Guevara-Aguirre and colleagues returned to the Ecuadorian families they had worked with in the past. They recruited 24 individuals with the syndrome and compared them to their unaffected relatives.
The results suggest that those with the growth-factor deficiency are no likelier to suffer from heart issues than their unaffected counterparts. If anything, the syndrome seems to be slightly protective against cardiovascular diseases. Affected individuals had lower blood pressure and glucose levels. They also had fewer issues with atherosclerosis, which is when plaque builds up in the arteries and begins to restrict blood flow. If left untreated, which is not uncommon since it is hard to notice, the plaque buildup can lead to heart attacks and strokes.
Same But Different: Not All Individuals With Laron Syndrome Share Protective BenefitsSomething worth noting is that not all individuals with Laron syndrome enjoy the same protective effects. Zvi Laron, professor emeritus at Tel Aviv University, was the first to recognize and define the syndrome in 1966 — that is why it carries his last name. But in the population that he studied, made up of consanguineous Jewish families from Yemen, a portion of the patients did develop an insulin intolerance and diabetes. Also, only a handful of individuals displayed the usual resilience against cancer seen in the Ecuadorian families with Laron syndrome.
How should we make sense of these discrepancies? Laron syndrome is caused by mutations to the growth hormone receptor gene, but these mutations can take many different forms. More or less of the gene may be affected, and in different areas. So even though all of the individuals in question suffer from the same syndrome, it may be brought on by subtly different mutations. Indeed, to date we know of 17 different genetic mutations that cause the disease. Based on the research of Zvi Laron, it seems that the protective benefits against cancer are only present when both parents share the same mutation in the same place and pass it on to their child, known as homozygosity.
The Ecuadorian community, whose roots can be traced back to Sephardic Jews who fled Spain during the Inquisition, all share the same mutation. It may just be that this particular mutation is the one that happens to grant longevity benefits. In which case, focusing on this community may prove most useful when it comes to the development of treatments that mimic the life-lengthening and disease-busting qualities of the syndrome.
ImplicationsAlthough Laron syndrome comes with clear challenges, it also seems to provide certain benefits. Those with the disorder, at least the Ecuadorian contingent, live longer and struggle with fewer age-related diseases than their unaffected counterparts. Most of these benefits can be traced back to lowered levels of insulin-like growth factor 1.
By studying the syndrome and learning more about its effects at the molecular level, we may discover ways of transferring the protective effects to the general population. The point here is not necessarily to grant longevity so much as to increase "healthspan," the number of years of your life you spend in good health. Indeed, Dr. Valter D. Longo —the senior author of the study— has experimented with different fasting-like diets that can reduce the levels of insulin-like growth factor 1 circulating in the body and along with it, various risk factors for disease. There are also molecules that block the protein, slowing down cancerous growths in the process. By fine-tuning these approaches, the protective effects of the syndrome might soon be available to everyone.
Genetic Mutations Leading To Truncated Proteins In Schaaf-Yang Syndrome
image:
From left to right, Mónica Centeno, Aina Prat, Juan Diego Gutiérrez, Susanna Balcells and Raquel Rabionet, members of the UB, the BUB, the IRSJD and the CIBERER.
view moreCredit: UNIVERSITY OF BARCELONA
Mutations in the MAGEL2 gene, which cause Schaaf-Yan syndrome (SYS) —an ultra-rare disease that affects neuronal and cognitive development— generate truncated, non-functional proteins that tend to accumulate in the cell nucleus. Moreover, this progressive accumulation of abnormal proteins could cause a toxic effect in patients affected by the syndrome, who suffer congenital malformations, intellectual disability, alterations in facial features, sleep apnoea and joint contractures.
These advances in SYS research appear in a study published in the Journal of Medical Genetics. The study was led by a team from the Faculty of Biology and the Institute of Biomedicine of the University of Barcelona (IBUB), the Sant Joan de Déu Research Institute (IRSJD) and the Rare Diseases Networking Biomedical Research Centre (CIBERER). This team is also the author of the publication of the first clinical guide on Schaaf-Yang syndrome (Journal of Medical Genetics, 2022), aimed at healthcare professionals and families of children affected by this pathology.
A better understanding of the function, genetic variants and impact of nuclear retention of the MAGEL2 protein will open new ways to design patient-specific gene therapies to prevent the synthesis of the altered protein and address SYS, a disease without treatment.
Genetic mutations leading to truncated proteins
The MAGEL2 gene is located on chromosome 15, is expressed in the nervous system and produces the MAGEL2 protein, which is involved in the retrograde transport and recycling of proteins in the cell cytoplasm of neurons. To date, more than eighty mutations in the MAGEL2 gene have been documented in the scientific literature, some of which are found repeated among patients. Currently, it is estimated that there are about 250 people diagnosed with Schaaf-Yang syndrome worldwide.
The new study, conducted with human cells in vitro, shows how almost all truncated proteins associated with Schaaf-Yang syndrome lose part of their molecular structure due to genetic mutations. "Functional MAGEL2 proteins have a complete molecular structure that allows them to interact with other proteins and carry out their normal biological functions. They are usually found in specific locations within the cytoplasm of the cell, mainly in subcellular compartments related to the transport and recycling of proteins", explains Susanna Balcells, professor at the UB's Department of Genetics, Microbiology and Statistics, and coordinator of the study. "In contrast — she continues — truncated proteins are shorter versions of the MAGEL2 protein, as they have been affected by genetic mutations. Therefore, truncated proteins lack certain regions necessary to function correctly in the cell".
Due to genetic mutations, truncated proteins lose key structural domains, such as the MAGE homology domain, which is crucial for interactions with other proteins. "The absence of this domain could prevent these essential interactions for the correct functioning of MAGEL2, such as its role in retrograde transport and protein recycling", explains Roser Urreizti.
When toxic proteins accumulate in the cell nucleus
Truncated proteins tend to accumulate inside the cell nucleus, and this could further aggravate the symptomatology of people affected by Schaaf-Yang. Mónica Centeno, "it is likely that, in a real cellular context, some of the truncated proteins synthesised can also be found in specific locations within the cytoplasm, such as endosomes, for example. However, as their structure is altered, they might not be able to perform their normal functions correctly".
The severity of clinical manifestations in those affected by Schaaf-Yang syndrome may be related to the accumulation of altered proteins in the cell nucleus. "In other words, the mutations that cause more severe symptoms also cause the truncated MAGEL2 protein to accumulate more in the nucleus. This could be explained by the fact that a higher accumulation of truncated proteins in the nucleus could be interfering with important nuclear processes and affect the functioning of the cell under normal conditions to a greater degree," says Raquel Rabionet.
Searching for treatments to address Schaaf-Yang syndrome
Cellular mechanisms that drive protein degradation — for example, the ubiquitin-proteasome system — could help reduce the negative effects of truncated proteins and contribute to mitigating the progression of the pathology. However, if the rate of protein production exceeds the degradation capacity of the cell, aberrant proteins may escape degradation and continue to exert toxic effects. The expert Aina Prat says that "in this regard, we have found that normal and truncated MAGEL2 proteins have very similar half-lives. Therefore, truncated MAGEL2 would be stable in the cell, where it could be exerting toxic effects".
"If we knew how truncated MAGEL2 proteins alter cell function, we could develop strategies to promote the degradation of these toxic proteins, restore cell function or compensate for the metabolic and signalling dysfunctions caused by their accumulation", concludes the team, which will drive further research to contribute to the development of innovative treatments for people affected by SYS.
JournalJournal of Medical Genetics
Method of ResearchExperimental study
Subject of ResearchCells
Article TitleSubcellular localisation of truncated MAGEL2 proteins: insight into the molecular pathology of Schaaf-Yang syndrome
Article Publication Date28-Mar-2024
Disclaimer: AAAS and EurekAlert! Are not responsible for the accuracy of news releases posted to EurekAlert! By contributing institutions or for the use of any information through the EurekAlert system.


Comments
Post a Comment