Deciphering My Myeloma Lab Results - HealthTree For AML

Mendelian Genetics: Patterns Of Inheritance And Single-Gene Disorders
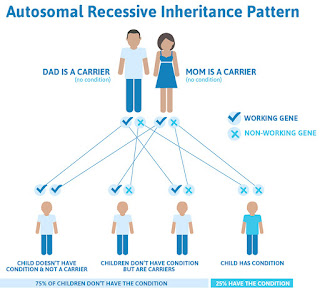
Autosomal recessive single-gene diseases occur only in individuals with two mutant alleles of the disease-associated gene. Remember, for any given gene, a person inherits one allele from his or her mother and one allele from his or her father. Therefore, individuals with an autosomal recessive single-gene disease inherit one mutant allele of the disease-associated gene from each of their parents. In pedigrees of families with multiple affected generations, autosomal recessive single-gene diseases often show a clear pattern in which the disease "skips" one or more generations.
Phenylketonuria (PKU) is a prominent example of a single-gene disease with an autosomal recessive inheritance pattern. PKU is associated with mutations in the gene that encodes the enzyme phenylalanine hydroxylase (PAH); when a person has these mutations, he or she cannot properly manufacture PAH, so he or she is subsequently unable to break down the amino acid phenylalanine, which is an essential building block of dietary proteins. As a result, individuals with PKU accumulate high levels of phenylalanine in their urine and blood, and this buildup eventually causes mental retardation and behavioral abnormalities.
The PKU-associated enzyme deficiency was determined biochemically in the 1950s—long before the PAH-encoding gene was mapped to human chromosome 12 and cloned in 1983. Specifically, Dr. Willard Centerwall, whose child was mentally handicapped, developed the first diagnostic test for PKU in 1957. Called the "wet diaper" test, Centerwall's test involved adding a drop of ferric chloride to a wet diaper; if the diaper turned green, the infant was diagnosed with PKU. The wet diaper test was used to reliably test infants at eight weeks after birth; by this time, however, infants who were affected by PKU had already often suffered irreversible brain damage.
Thus, in 1960, Dr. Robert Guthrie, whose niece suffered from PKU and whose son was also mentally handicapped, established a more sensitive method for detecting elevated phenylalanine levels in blood, which permitted a diagnosis of PKU within three days after birth. Guthrie's test used bacteria that were unable to make their own phenylalanine as messengers to report high blood levels of phenylalanine in an infant's blood sample obtained via heel prick. With Guthrie's method, the phenylalanine-deficient bacteria were grown in media together with a paper disk spotted with a drop of the infant's blood. If the phenylalanine levels in the blood were high, the bacteria would grow robustly, and a diagnosis of PKU could be made. Through the ability to discover that their child had PKU at such an early age, parents became able to respond immediately by feeding their child a modified diet low in proteins and phenylalanine, thereby allowing more normal cognitive development. Guthrie's test continues to be used today, and the practice of obtaining an infant's blood sample via heel prick is now used in numerous additional diagnostic tests.
Several other human diseases, including cystic fibrosis, sickle-cell anemia, and oculocutaneous albinism, also exhibit an autosomal recessive inheritance pattern. Cystic fibrosis is associated with recessive mutations in the CFTR gene, whereas sickle-cell anemia is associated with recessive mutations in the beta hemoglobin (HBB) gene. Interestingly, although individuals homozygous for the mutant HBB gene suffer from sickle-cell anemia, heterozygous carriers are resistant to malaria. This fact explains the higher frequency of sickle-cell anemia in today's African Americans, who are descendants of a group that had an advantage against endemic malaria if they carried HBB mutations. Finally, oculocutaneous albinism is associated with autosomal recessive mutations in the OCA2 gene. This gene is involved in biosynthesis of the pigment melanin, which gives color to a person's hair, skin, and eyes.
XORTX Initiates Precision Medicine Program
CALGARY, Alberta, Oct. 09, 2024 (GLOBE NEWSWIRE) -- XORTX Therapeutics Inc. ("XORTX" or the "Company") (NASDAQ: XRTXTSXV: XRTXFrankfurt: ANU), a late-stage clinical pharmaceutical company focused on developing innovative therapies to treat progressive kidney disease, is pleased to announce the Company has initiated a precision medicine program. On August 29, 2024, XORTX announced that independent peer-reviewed research reported that genetic factors are linked to the over-expression of xanthine oxidase ("XO") and play a role in several diseases, including kidney disease. These ground-breaking findings provide an opportunity to expand the Company's programs and approach by combining genetic diagnostics focused on treating kidney and diseases such as sepsis by inhibiting XO with xanthine oxidase inhibition targeting individuals most in need.
Recent pioneering discoveries provide XORTX with the opportunity to develop diagnostics that identify specific genetic factors. These diagnostic tools alongside XORTX's expertise at developing unique formulations of uric acid lowering agents and XO inhibitors will permit XORTX to tailor treatments to subpopulations of individuals that have common susceptibility or similar response to a particular drug.
Dr. Allen Davidoff, PhD., Chief Executive Officer of XORTX commented, "The application of genetic diagnostic tools and recent pioneering discoveries in autosomal dominant polycystic kidney disease ("ADPKD"), diabetic kidney and non-diabetic kidney disease provide a unique opportunity that XORTX is ideally positioned to address. The new opportunity to specifically identify a series of genetic factors, then targeting XO has enormous therapeutic potential for treating the health consequences associated with these alleles. The Company will begin evaluating individuals as early as our planned registration clinical trial in patients with ADPKD providing XORTX with an opportunity to better understand the role these genetic factors play in progressive kidney disease." About Xanthine Oxidase:
Xanthine oxidase is an essential enzyme within the uric acid metabolic pathway and is required for the breakdown of purine nucleotides. The breakdown products of XO, uric acid (UA) and reactive oxygen species (ROS), are released during the enzymatic reaction and may play a detrimental role in the circulatory system and within tissue during disease. XORTX sponsored discoveries in rodent models of polycystic kidney disease ("PKD") implicate over-expression or over-activity of XO as a potentially important target in treating this disease.
Recent evidence for the over expression of Xanthine Oxidase in Disease:
Evidence for over-expression of XO in human PKD has not been reported to date, although work by Wang et al. Suggests linkage of genetic factors to PKD(1). Recently, new emerging discoveries link genetic factors to specific populations and show that higher XO expression is associated with a variety of conditions including hyperuricemia(2), sepsis, organ failure and sepsis associated acute respiratory distress syndrome (ARDS)(3,4), kidney dysfunction(3, 4), diabetes(5), polycystic kidney disease(1,5) and kidney failure(6,7). From a mechanistic standpoint, these studies advocate for a precision-medicine approach in which genetic risk variants would guide treatment decisions(1).
References:
About XORTX Therapeutics Inc.
XORTX is a pharmaceutical company with two clinically advanced products in development: 1) our lead, XRx-008 program for ADPKD; and 2) our secondary program in XRx-101 for acute kidney and other acute organ injury associated with Coronavirus / COVID-19 infection. In addition, XRx-225 is a pre-clinical stage program for Type 2 Diabetic Nephropathy. XORTX is working to advance its clinical development stage products that target aberrant purine metabolism and xanthine oxidase to decrease or inhibit production of uric acid. At XORTX, we are dedicated to developing medications to improve the quality of life and future health of patients. Additional information on XORTX is available at www.Xortx.Com.
For more information, please contact:
Allen Davidoff, CEO adavidoff@xortx.Com or +1 403 455 7727 Nick Rigopulos, Director of Communicationsnick@alpineequityadv.Com or +1 617 901 0785Neither the TSX Venture Exchange nor Nasdaq has approved or disapproved the contents of this news release. No stock exchange, securities commission or other regulatory authority has approved or disapproved the information contained herein.
Forward Looking Statements
This press release contains express or implied forward-looking statements pursuant to applicable securities laws. These forward-looking statements include, but are not limited to, the Company's beliefs, plans, goals, objectives, expectations, assumptions, estimates, intentions, future performance, other statements that are not historical facts and statements identified by words such as "expects", "anticipates", "intends", "plans", "believes", "seeks", "estimates" or words of similar meaning. These forward-looking statements and their implications are based on the current expectations of the management of XORTX only, and are subject to a number of factors and uncertainties that could cause actual results to differ materially from those described in the forward-looking statements. Such risks, uncertainties, and other factors include, but are not limited to, our ability to obtain additional financing; the accuracy of our estimates regarding expenses, future revenues and capital requirements; the success and timing of our preclinical studies and clinical trials; the performance of third-party manufacturers and contract research organizations; our plans to develop and commercialize our product candidates; our plans to advance research in other kidney disease applications; and, our ability to obtain and maintain intellectual property protection for our product candidates. Except as otherwise required by applicable law and stock exchange rules, XORTX undertakes no obligation to publicly release any revisions to these forward-looking statements to reflect events or circumstances after the date hereof or to reflect the occurrence of unanticipated events. More detailed information about the risks and uncertainties affecting XORTX is contained under the heading "Risk Factors" in XORTX's Annual Report on Form 20-F filed with the SEC, which is available on the SEC's website, www.Sec.Gov (including any documents forming a part thereof or incorporated by reference therein), as well as in our reports, public disclosure documents and other filings with the securities commissions and other regulatory bodies in Canada, which are available on www.Sedarplus.Ca.
What Is Early Onset Familial Alzheimer Disease (eFAD)?
By Gabrielle Strobel
Definition: What Is eFAD?
Early onset familial Alzheimer disease (eFAD) is hereditary and marked by Alzheimer disease symptoms that appear at an unusually early age. Symptoms can start in a person's thirties, forties, and fifties (and very rarely in the late twenties). Generally, if you are diagnosed with eFAD, then one of your parents will also have had it if he or she lived long enough, and your siblings and your children may have a 50-50 chance of having inherited it. Very rarely, eFAD can make a first-time appearance in a family through a new genetic mutation.
Genetics researchers studied eFAD families to discover the three known genes that cause familial AD: amyloid precursor protein (APP), presenilin-1 (PS1), and presenilin-2 (PS2). Of these, PS1 mutations account for most eFAD, while APP and PS2 are more rare. Having a pathogenic mutation in one of these three genes virtually guarantees that one will develop early onset Alzheimer disease. Tests can determine which gene is at fauly (see Diagnosis). There are also cases of eFAD that cannot be linked to one of these three genes. There may be additional genes waiting to be discovered, if only researchers could connect with more eFAD families.
Like the more common late-onset AD, eFAD is incurable. Over several years, the patient will lose memory and other mental functions, and become completely dependent on others. At this time, there is no treatment to slow down the disease. Ironically, eFAD patients often have been excluded from drug studies because of their young age, even though studies of these families have contributed to some of the most important findings about Alzheimer disease, including its very discovery (see "How Early Onset Dementia Led to a Historic Discovery") and, later, discovery of the genes causing it. By raising awareness of eFAD, we hope families will know they are not alone, and that researchers will do more to involve them in the search for treatments.
Prognosis: Is eFAD Different from LOAD?
Neurologists generally agree that eFAD and late-onset AD are essentially the same disease, apart from the differences in genetic cause and age of onset. EFAD progresses with the same overall sequence of symptoms and increasing impairments as LOAD. From the neurologist's perspective, two things stand out the most about eFAD, says Dennis Selkoe of Harvard Medical School. One is how pure the AD clinical syndrome develops in an otherwise healthy person (see Diagnosis), and the other is how high a burden the disease imposes on the spouse and children, who are often still young. These patients are active, working people who are in the midst of building a life for their families. Early onset FAD is acutely tragic because the patient faces a relentless and progressive loss of brain function so prematurely, while he or she is still physically vigorous. As a result, eFAD is often accompanied by psychiatric complications such as depression and agitation.
While eFAD and LOAD are outwardly the same, the underlying process that leads to eFAD is distinct from that which results in LOAD. As a genetic disorder, eFAD clearly is the consequence of the malfunctioning of the mutated genes, whereas late-onset disease is more likely due to a gradual accumulation of age-related malfunctions. Some studies have noted that the pathologic hallmarks (protein deposits called plaques and tangles) are more severe in eFAD than LOAD, and may be concentrated in different regions. These differences in underlying mechanism suggest that treatments for eFAD may overlap with, but not always be identical to, treatments being developed for LOAD.
How Common Is Early Onset Familial Alzheimer Disease?
The medical literature estimates that between 1 and 5 percent of all Alzheimer cases are early onset. This includes familial and sporadic forms, and translates into 50,000 to 250,000 people in the U.S. A report issued by the Alzheimer's Association in March 2007 puts the number of people with AD who are younger than 65 at around 200,000 (Alzheimer's Disease Facts and Figures [.Pdf]), a large number than more visible neurodegenerative diseases such as ALS (Lou Gehrig disease) and Huntington disease.
When put to AD researchers, however, the simple question of how many people have eFAD generates a lengthy discussion. Why the uncertainty? For one thing, the answer depends on how one defines early onset familial AD. For another, definitive data do not exist. The section below explains how scientists derive the numbers that are known to date, and why they have not yet been able to deliver precise counts. In short, the reasons boil down to the complexity of AD genetics, the difficulty of compiling family pedigrees, and misdiagnosis of AD in younger people for depression and other illnesses.
For practical and research purposes, doctors and scientists need defined populations for study and the numbers change based on the definitions. The definition would seem to rest on two criteria:
By these criteria, Alzheimer disease can be sliced into four subcategories:
Early onset AD (EOAD) Late-onset AD (LOAD) Genetic Early onset familial (eFAD) Late-onset familial Sporadic Early onset sporadic Late-onset sporadicIn reality, however, Alzheimer disease exists in a continuum, a mix of gradations across these definitions. Also, each subtype of AD is not a pure form unto itself. For example, a family is categorized as either early onset or late-onset AD, but new research shows that about a quarter of families with LOAD also have a relative who develops EOAD (Brickell et al., 2006).
A diagnosis of AD in the thirties, forties, and fifties clearly is considered EOAD and past 75 it is LOAD, but there is no consensus on exactly where to place the cutoff. Formal diagnostic texts put it at age 65; but some investigators prefer 60 and use that age in their research. Most large epidemiological studies don't assess eFAD separately with the standard tools of prevalence (percentage of the population who have a disease at any given time) and incidence (percentage of people who get it every year) because those numbers are very low, and large epidemiology studies of dementia rarely capture people below 65. Because population-based epidemiology numbers are few and far between, scientists instead work with estimates generated from patient counts in clinical settings, and that is where the 1 to 5 percent figure comes from. The wide range stems from local differences, such as different referral patterns and levels of specialization.
Some epidemiologists note that 5 percent of all AD (i.E., around 250,000 U.S. Cases) might overstate the true number of eFAD cases because a larger fraction of old people than young people who develop AD may not be diagnosed, and therefore not counted in the statistics. Losing one's mental abilities at 50 is such a dramatic event that people eventually find their way to a neurological clinic and get counted, more so than when it happens in one's eighties. On the other hand, some neurologists hesitate to diagnose AD in people under 60, driving numbers of early onset cases down. And the number of early onset cases among the tens of millions of people in the U.S. Who have no health insurance is unknown, especially in remote rural areas where health care services are sparse and access is a problem. Given these uncertainties, researchers generally accept 2 to 3 percent of all AD (i.E., roughly 100,000 U.S. Cases) as a conservative estimate.
The second criterion for measuring forms of AD—familial versus sporadic—also is more complicated than it appears at first sight. The term familial implies that at least two generations of a family have AD. Familial AD can occur with early onset and late onset, but the precise number is unclear. That is because familial AD is not always caused by the clear-cut inheritance of a single gene, but may cluster in families by way of a more murky genetic pattern, where several unlucky genes may add up in their effects on the body to drive down AD's age of onset. This form is more difficult to identify, and so the numbers of affected families are not accurately counted.
Scientists do not fully understand the relative contributions of genetics and the environment to AD, but they believe that there is a spectrum. The later the onset of AD, the more aging and environmental factors are thought to dominate and the smaller a person's genetic predisposition appears to be. The earlier the age of onset, the more likely AD is to be driven by a deterministic, powerful mutation in a single gene that gets passed on through generations. This kind of AD inheritance is like that of quintessential genetic diseases, such as hemophilia, or classic traits of textbook genetics, such as the color of Gregor Mendel's garden peas. The familial mutations reported in the scientific literature (see AD/FTD mutation database and Alzforum mutations list) are of this kind. The middle of the gene-environment spectrum is much more hazy, and it is the subject of intense research. Many candidate genes are being scrutinized, but none are clearly understood. Scientists do not yet know how the genes interact with one another or with environmental factors to create a burden of AD risk in a given person. Overall, epidemiologists estimate the heritability of AD in this middle category to be approximately 80 percent.
Autosomal-dominant forms of eFAD result from mutations in one of three genes. They are APP on chromosome 21, presenilin-1 on chromosome 14, and presenilin-2 on chromosome 1. Of these, presenilin-1 is by far the most common cause of eFAD. Another gene, ApoE, is known to increase the likelihood that a person will develop AD when it comes in the form known as ApoE4. However, it does not cause autosomal-dominant disease like the three genes described above. Rather, ApoE4 is a risk factor. It is important to be aware of the difference between a deterministic mutation and a genetic risk factor. Very few carriers of known pathogenic APP or presenilin mutations live past middle age without developing AD, whereas many people who carry two ApoE4 copies do. In other words, a finding of a pathogenic APP or presenilin mutation constitutes a genetic diagnosis. A finding of two ApoE4 alleles does not; it simply means that the person's odds of developing AD are increased by about 12- to 15-fold. Scientists think that ApoE4 lowers the age of onset by about a decade from when that person would have otherwise developed AD. (People without ApoE4 tend to die of other causes before they are old enough to get AD.) In a given family with an APP or presenilin-2 (but not presenilin-1) mutation, carriers who also have inherited an ApoE4 gene tend to get sick at a younger age than their relatives who have the more neutral ApoE3 or the somewhat protective ApoE2 version alongside the APP or presenilin mutation.
Some families with early onset AD know which genetic mutation is responsible for their disease, but more do not. The three known AD genes together explain only half of all early onset AD. Frequently, neurologists at referral centers will see people with early onset AD who have no family history; those are called sporadic cases. Of these, some people, upon genetic testing, turn out to have a previously identified mutation in one of the three dominant genes. Others prove to have a different mutation in one of the three genes. More often, however, geneticists cannot pin down a cause, so the story of that person's, or family's disease awaits the discovery of new AD genes.
Another frequent situation is that affected patients or their caregivers can tell their doctor fragments of a family history but not enough detail for a geneticist to puzzle out if the disease is truly familial in origin, much less which gene could be at fault. Typically, the caregiver of a young person with AD may know of one parent who had it but died, plus perhaps stories about some relatives back in the family's country of origin. Incomplete family information is one reason why, despite the large number of individual early onset AD cases, geneticists have been able only in relatively few instances to piece together the multi-generational pedigrees that form the basis for identifying disease genes.
After a thorough clinical evaluation to establish the presence of clinical AD (see Diagnosis), the first thing a knowledgeable clinician will try to do when AD looks familial is to establish the patient's family tree to trace the pattern of inheritance. In some cases, families are so motivated to better understand their disease that they undertake the genealogy themselves, said Nick Fox of the Dementia Research Center at London's University College. In other instances, delicate family dynamics can stymie the gene sleuth. A U.S. Physician described a case where a patient with obvious early onset AD had two healthy parents and looked entirely different from his siblings. "I suspected non-paternity, but could not pursue the possible familial source of this patient's AD," the physician said. "If the family did not know of the non-paternity, they wouldn't want to find out at that stage in life through me."
Another reason why eFAD numbers are vague is that neurologists and psychiatrists may hesitate to diagnose AD in young or middle-aged people. Some are insufficiently aware of eFAD, while others hold off on diagnosing it exactly because it is considered very rare. In effect, eFAD gets passed off for something else and proper diagnosis is delayed until the patient is older, said Thomas Bird of the University of Washington, Seattle. Frequently that something else is depression (for a personal account, see interview). Yet other doctors are misled by variations in how eFAD presents (see Diagnosis). Confusingly, familial AD sometimes shows up in one family member in his/her thirties and in another in the sixties, although in a majority of families disease begins in the forties and early fifties. In rare instances, disease can show up in different guises in different members of a single family. For example, in one case a family member exhibited weakness and gradual paralysis of the legs and only minor dementia, while another had pure AD. Such variations probably are the result of secondary genes that somehow modify the effect of the original AD mutation to push onset back or forward, or to create a different combination of symptoms.
All told, researchers in the field suspect that an additional one to three genes causing eFAD remain to be found, plus several more that influence the age at which AD strikes. Knowing more genes may eventually help scientists get a better grasp on defining eFAD, but to be able to pinpoint them, scientists need more families willing to participate in research. To date, the available collections of families with AD willing to participate in research have been large enough only to identify genes that either have strong effects or that occur relatively frequently. For genes that affect one's AD risk weakly, and for less common genes, larger samples of patients and healthy relatives will be needed.
To date, families with eFAD have been viewed as exceedingly rare exceptions, too rare to include in clinical studies and drug trials. In one sense, this makes eFAD the ultimate orphan disease; it lacks the visibility, funding, and advocacy groups associated with diseases such as Huntington disease and ALS, even though the numbers affected by early onset AD are comparable or greater.
NEXT: How Early Onset Dementia Led to a Historic Discovery


Comments
Post a Comment