Deciphering My Myeloma Lab Results - HealthTree For AML

Fragile X Syndrome
Fragile X syndrome, also known as Martin-Bell syndrome, is a genetic condition that affects a child's learning, behavior, appearance, and health. Symptoms can be mild or more severe, and boys often have a more serious form of the condition than girls.
Children born with this condition have developmental concerns, including learning disabilities and limits to mental functions. Special education and therapy can help with learning and developing skills according to their ability. Medications and other treatments can improve their behavior and physical symptoms.
Fragile X syndrome is a condition that affects a child's learning, behavior, appearance, and health. Children born with the condition have developmental concerns that can include learning disabilities and limits to mental functions. Special education and therapy can help with learning and developing skills, and medication and other treatments can improve their behavior and physical symptoms. (Photo Credit: E+/Getty Images)
People with fragile X may have several symptoms, including:
About 40% of individuals with fragile X also have autism.
If your child has both fragile X and autism, they're more likely to have seizures, sleep issues, more behavioral issues, and need more medications.
Almost 80% of children with fragile X also have attention deficit disorder (ADD) or attention deficit hyperactivity disorder (ADHD).
Some children with fragile X also have changes to their face and body that can include:
Signs of fragile X usually start with delayed speech and language trouble by the age of 2, along with delays in motor milestones. Boys are usually diagnosed around the age of 35-37 months. Girls are diagnosed around 42 months old. Symptoms are usually milder in girls. While most boys with fragile X have trouble with learning and development, girls usually don't have these issues.
Girls with fragile X sometimes have trouble getting pregnant when they grow up. They might also go into menopause earlier than usual.
The condition can also cause problems with:
Fragile X syndrome is passed down in families through a mutation in the FMR1 gene. The FMR1 gene, which is on the X chromosome, makes a protein called FMR that helps nerve cells talk to one another. A child needs this protein for their brain to develop normally. Children with fragile X make too little or none of it.
People with this condition also have more copies than usual of a DNA segment known as CGG. In most people, this segment repeats 5 to 40 times. In people with fragile X, it repeats more than 200 times. The more times this DNA segment repeats, the more serious the symptoms are.
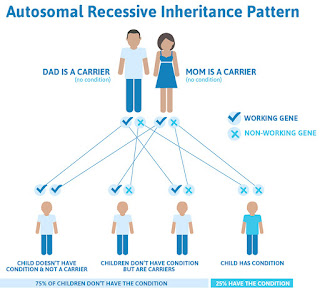
A mother with the FMR1 gene change has a 50% chance of passing it to any of her children. A father can only pass it to his daughters.
Since the FMR1 gene is on the X chromosome, it is known as an X-linked condition. That means that all males who carry the gene mutation develop symptoms. As a result, boys are more likely to have fragile X than girls and often show more severe symptoms. Girls have two copies of the X chromosome, so even if one X chromosome has the gene change, the other copy can be fine.
About 1 in 151 females and 1 in 468 males carry something known as the FMR1 premutation. That means that their CGG segment repeats anywhere from 55 to 200 times. These pre-mutations usually don't impact their health, and they don't show symptoms. But people with pre-mutations can still pass the gene change on to their children. This gene can also change size as it passes from parent to offspring. This means it eventually could develop into a full-blown mutation.
The number isn't clear, but about 1 in 8,000 to 11,000 females have fragile X syndrome, while 1 in 4,000 to 7,000 males have the condition.
There aren't any risk factors for fragile X that you can control. If you have the FMR1 gene, your child could have it, too.
While there's no way to prevent fragile X syndrome, you may want to consider genetic testing.
These tests can be done during pregnancy to see if an unborn baby has fragile X:
After the child is born, a blood test can diagnose fragile X syndrome. This test looks for the FMR1 gene change.
Babies born with fragile X syndrome don't always show signs of it. The doctor might notice that the baby's head is larger than usual. As the child gets older, learning and behavior problems can start.
There are other reasons why adults may want to request fragile X testing. They include:
No medicine can cure fragile X. Treatments can help your child learn more easily and manage problem behaviors. The earlier you start it, the better. Options include:
Special education. Your child will need extra help with learning. It's important to set up an IEP or 504, which are education plans that guide the school in providing support. Your school may also provide:
Changes to surroundings. You'll want to make sure your child's environment, at home and at school, is set up for success. Some ways to do this include:
Medications. There are no medications to cure Fragile X. There are, however, different drugs that can help manage symptoms. Options include:
Many fragile X clinics have opened in the U.S. They can keep parents up-to-date on the latest research, including medications that may be newly available or in clinical trials. The National Fragile X Foundation can be a helpful resource in finding a clinic.
Fragile X syndrome can cause the following health complications:
Fragile X syndrome can also lead to learning and developmental conditions, such as intellectual disability, ADHD, aggression, and autism.
Many adults with fragile X syndrome require a high level of support in adulthood. About a third of women with fragile X can live independently, and almost half are able to have a full-time job. But only about 10% of men with fragile X can live on their own, and only about 20% have a full-time job.
Most people with a fragile X premutation don't show any symptoms. But some go on to develop a fragile X-associated disorder. The two most common conditions are:
Fragile X-associated primary ovarian insufficiency (FXPOI). Women with FXPOI go through menopause before the age of 40. They may also experience infertility.
Fragile X-associated tremor/ataxia syndrome (FXTAS). This is a nervous system disorder that can happen in older adults. It can cause:
The symptoms of fragile X aren't life-threatening. Your life expectancy with the condition is the same as that of anyone without it.
A lot of people with the condition are able to live successful lives on their own. About 8 in 20 women and 1 in 20 men with fragile X don't need help with daily activities.
Depending on the severity of fragile X, people with the condition can go to school, have conversations, read books, learn new ideas, and finish other tasks by themselves.
To learn more about fragile X syndrome, join a support group. You may also reach out to an organization like the National Fragile X Foundation for advice and resources.
There, you can learn about local events and groups for people with fragile X.
There are also resources for parents. If you recently found out that your child has fragile X, this site offers many tips, videos, and firsthand experiences to help you understand how to care for them.
Fragile X syndrome is a genetic condition that causes intellectual and developmental disability. It is more severe in males than in females. People with fragile X syndrome are also more likely to develop autism.
There aren't any risk factors for fragile X that you can control. If you have the FMR1 gene, your child could have it, too. It's diagnosed through genetic testing.
There's no "cure" for fragile X syndrome, but most people with it respond well to speech, occupational, and behavioral therapy. Some adults with fragile X syndrome are able to live independently and hold a full-time job. Others need more support. Many people with fragile X syndrome go on to lead long, fulfilling lives.
What kind of mutation is fragile X syndrome?
It's a genetic mutation. People with fragile X syndrome have changes in their FMR1 gene, which is on the X chromosome. It makes a protein called FMR that helps nerve cells talk to one another. People need this protein for their brains to develop normally. Individuals with fragile X make too little or none of it. They also have more copies than usual of a DNA segment known as CGG. In most people, this segment repeats 5 to 40 times. In people with fragile X, it repeats more than 200 times. The more times this DNA segment repeats, the more serious the symptoms are.
Is fragile X like autism?
People with fragile X have a higher incidence of autism than those without the condition. If your child has both fragile X and autism, they're more likely to have seizures, sleep issues, more behavioral issues, and need more medications.
What are the behaviors of fragile X syndrome?
People with fragile X syndrome have many different behaviors. Some of the more challenging ones include:
But those with fragile X have plenty of behavior strengths, too. They're great at imitation and have strong visual memories. People with fragile X can also be very social, and they like to help others.
What Is Rett Syndrome?
Rett syndrome (RTT) is a rare, severe, and progressive disorder that mostly affects girls of all races. It can impact your child's ability to speak, walk, eat, or breathe easily. It was named after Andreas Rett, an Austrian pediatrician, who was the first person to report on the condition.
Parents or doctors usually notice signs of RTT within the first 2 years of a child's life. If your child has the condition, they often miss key milestones in development (such as walking or talking) or lose abilities they used to have.
There's no cure for this lifelong disorder, but early treatment may help your child adjust.
Most children with Rett syndrome have a mutation on the X chromosome, usually in a gene called MECP2. MECP2 is present in more than 95% of Rett cases.
It isn't clear what exactly this gene does or how its mutation (change) leads to the condition. Researchers think that the single gene may influence many other genes involved in development. That's why two girls with the same mutated gene might have very different symptoms.
Two other genes, CDKL5 and FOXG1, are associated with variations of RTT.
Although Rett syndrome is genetic, children rarely inherit the faulty gene from their parents. Rather, it's a chance mutation that happens in DNA.
Rett syndrome genetic testing
A blood test can confirm whether the MECP2, CDKL5, or FOXG1 genes are present. This can be useful to determine if your child has RTT when they show the symptoms.
You can also be tested if there's a family history of the condition. Prenatal testing can check if a second child might have RTT. However, it's unlikely anything will turn up since the condition is nearly always random. The chance of having a second child with the condition is less than 1% unless the mother already has the MECP2 gene or one of the variants, which is uncommon.
Still, you and your partner can get tested for gene mutations before you decide whether you want to have more kids. You can get more information by talking with an experienced genetic counselor.
If a mother learns that she has an MECP2 mutation (without symptoms, just a positive blood test), her daughters who don't have Rett syndrome can choose to get tested once they become old enough to have kids. It could help them find out if they also carry the mutated gene. But even if one daughter has Rett, it's very unlikely that a sister would carry the gene as well.
Both conditions can make it hard to communicate and socialize.
But there are key differences:
About 1 in every 10,000-15,000 girls worldwide are born with Rett syndrome. The disorder is even rarer in boys.
RTT is often misdiagnosed, so it could be more common than we think.
When boys develop the Rett syndrome mutation, they rarely live past birth. Males have only one X chromosome (while girls have two), so the effects of the genetic mutation are much more serious and almost always fatal.
Most baby boys with RTT show signs of it very early on, and they have health problems at birth or soon after. They need aggressive medical treatment, meaning treatment that's more intense than usual.
The age when symptoms appear varies. Most babies with Rett syndrome seem to grow normally for the first 6 months before any signs of the disorder become obvious. Researchers once thought that children with RTT never showed any symptoms before 6 months. But more recent studies have shown that they sometimes have symptoms from birth.
The most common changes usually show up when babies are between 12 and 18 months of age, and they can be sudden or progress slowly.
Some symptoms of RTT include:
Slowed growth. The brain doesn't grow properly, and the head is usually small — doctors call this microcephaly. This stunted growth becomes clearer as your child gets older.
Problems with hand movements. Most children with Rett syndrome lose the use of their hands. They tend to wring or rub their hands together or bring their hands to their mouths.
No language skills. Between the ages of 1 and 4, social and language skills start to decline. Children with RTT stop talking and can have extreme social anxiety. They may stay away from or not be interested in other people, toys, and their surroundings.
Problems with muscles and coordination. This can make walking awkward. It also affects the ability to chew and swallow.
Trouble breathing. This can include very fast breathing (hyperventilation), forceful exhaling of air or saliva, and swallowing air.
Seizures. Most people with Rett syndrome have seizures at some point in their lives.
It's also possible to have:
Behavior changes. Children with RTT tend to become tense and irritable as they get older. At times, they may cry or scream for a while or have long fits of laughter. Some kids also make unusual faces, lick their hands, or grasp at hair or clothes.
Unusual eye motion. This can include staring or blinking intensely, crossing eyes, or shutting one eye at a time.
Trouble sleeping. Your child might have a hard time falling asleep at night and nod off during the day. Or they might wake up at night screaming or crying.
Scoliosis. This sideway curve in the spine is common with Rett syndrome. It usually starts when a child is between 8 and 11 years old and gets worse with age. If it becomes severe, your child may need surgery.
Irregular heartbeat. Many children and adults with RTT have this serious condition, which can be life-threatening without treatment.
It's possible to have a few other symptoms, such as:
Symptoms usually don't improve over time. They often get worse very slowly or don't change. It's rare for people with RTT to be able to live on their own.
In general, there are four stages. But the way the stages unfold and the severity of RTT vary from child to child.
Stage I: Early onset
This stage usually happens when your baby is between 6 and 18 months of age. It lasts a few months to a year.
The symptoms of the disorder are subtle and can be easy to miss. Your baby might make less eye contact with you and seem less interested in toys. They might also take longer than usual to sit up or crawl.
Stage II: Rapid destructive
Some doctors also call this the "rapid deterioration" stage. It usually starts when a child is 1 to 4 years old, and it can last weeks to months.
During this stage, your child could lose the skills they used to have. It can happen quickly or gradually.
You might also notice clearer symptoms of Rett syndrome, like slower head growth, unusual hand movements, rapid breathing, trouble moving or coordinating, and losing social and communication skills.
Stage III: Plateau
This stage can start anytime from preschool to adulthood, and can last for decades. Most of your daughter's life is in this stage.
She may continue to have trouble moving, but she may cry and get irritable less often. Communication skills and hand use might also improve.
She may start to have seizures during this stage. In general, children with Rett syndrome don't get seizures before they're 2 years old.
Stage IV: Late motor deterioration
Your child may move less on their own or not at all. She may also have muscle weakness, limited range of motion in her joints, and scoliosis, which may require a back brace or surgery.
Hand movements and breathing problems may improve a bit or stay stable. If she has seizures, she may get them less often, too.
Doctors can make the diagnosis by observing your child's pattern of symptoms and behavior. They'll probably also ask you about things such as when the symptoms started.
Because RTT is rare, doctors will first rule out other conditions, including autism spectrum disorder, cerebral palsy, metabolic disorders, and prenatal brain disorders.
Genetic testing can help confirm the mutation in 80% of girls with suspected Rett syndrome. Doctors also rely on what's called an RTT Diagnostic Criteria Worksheet. It assesses your child's early growth and development.
A diagnosis of Rett syndrome shouldn't solely be based on genetic testing because the mutation can be seen in other similar conditions.
There's no cure for RTT, but treatments can help with a child's symptoms. They should get these treatments for their entire life.
The best treatment options for Rett syndrome include:
Standard medical care and medication
Meds may help control symptoms such as seizures, stiff muscles, and problems with sleeping, breathing, the heart, or digestive tract.
In 2023, trofinetide (Daybue) became the first FDA-approved drug to treat adults and children over 2 with Rett syndrome. Daybue can't cure RTT, but it improves many of the symptoms.
Physical therapy
Physical therapy and using braces or casts can help children who need hand or joint support or who have scoliosis. Physical therapy can help them keep moving, sit more easily, walk better, and improve their balance and flexibility. Assistive devices such as walkers or wheelchairs might also help.
Speech therapy
If your child has trouble talking, this could help them learn nonverbal ways to communicate and socialize.
Occupational therapy
This can boost your child's ability to use their hands to do things such as putting on clothes and feeding themselves. If they have to make repetitive movements with their arms and hands, the occupational therapist might recommend splints that limit elbow and wrist motion.
Good nutrition
Work with your child's doctor to make sure they're eating a balanced diet, which is important for healthy growth and better mental, physical, and social skills. Also, ask the doctor what you need to do to prevent your child from choking on food or vomiting while eating. Some children and adults with RTT benefit from being fed through a tube placed into the belly.
Behavioral therapy
This might help if your child has certain behavior issues. It could also teach them good sleep habits that help them get a better night's rest.
Supportive services
You can look into early intervention programs as well as school, social, and job-training services for your child.
Each child with RTT will have different symptoms. Some may have a mild version of the disorder, while others have it more severely. Problems with walking and other motor skills may get worse over time, while other problems such as seizures and communication may improve.
It's likely that your child will need help with feeding, bathing, dressing, and going to the toilet, but may eventually be able to do some of these things for themselves. You'll probably have to lift your child or help her walk. You and your daughter may need the help of a device to communicate. But she can still express a wide range of emotions and take part in many activities. Some kids may be able to go to school and learn how to socialize better.
Rett syndrome life expectancy
Many girls with Rett syndrome can live at least into middle age. The leading cause of death is cardiorespiratory issues (issues with the heart and lungs). Researchers are studying women with the disease, which was only widely recognized in the last 30 years.
Current research on Rett syndrome is focused on gene therapy. Scientists are trying to figure out a way to substitute the malfunctioning MeCP2 gene, as well as to locate other genes that may be involved in RTT.
Support groups for Rett syndrome
Support groups for parents and other caregivers of children with RTT can be very helpful, especially since the disease is so rare and you may not know of another person with it in your circles. The International Rett Syndrome Foundation (IRSF) runs several Facebook groups for parents, siblings, single mothers, and others who have a loved one with RTT. For more information, go to the IRSF Connect website. Another support resource is Girl Power 2 Cure.
Rett syndrome (RTT) is a rare disorder that mostly affects girls. Babies who have it are normal for the first year to 18 months of life, and after that, they start regressing. They may stop walking and communicating, do repetitive hand motions, and have trouble with breathing, chewing, and swallowing. RTT is caused by the MECP2 gene on the X chromosome. Although there is no cure, the first drug to control symptoms is now available.
Is Rett syndrome dominant or recessive?
It's an X-linked dominant mutation.
Do girls with Rett syndrome get periods?
Yes, they get periods at the same ages and for the same durations as most girls without Rett syndrome. Some girls with RTT use sanitary pads or tampons. Others take birth control pills or injections to reduce or eliminate their periods.
Is there a cure for Rett Syndrome?
No, there's no cure, yet. But there are a lot of therapies and medications to help people with the condition have a good quality of life.
Gene Therapy News
May 30, 2024 — Researchers have developed a novel version of a key CRISPR gene-editing protein that shows efficient editing activity and is small enough to be packaged within a non-pathogenic virus that can deliver ...
May 29, 2024 — Bioengineers report that a foaming liquid worked better than a standard liquid formulation at transferring gene therapy components to cells in laboratory ...
Apr. 30, 2024 — In an effort to improve delivery of costly medical treatments, a team of researchers in electrical engineering has developed a stimulating method that could make the human body more receptive to ...
Apr. 24, 2024 — In a proof-of-concept study, researchers demonstrated the effectiveness of a potential new therapy for Timothy syndrome, an often life-threatening and rare genetic disorder that affects a wide range ...
Apr. 22, 2024 — Clarifying the cause of a skin disease led to the discovery of a new disease-causing gene, a new category of diseases, and new perspectives for both counseling and therapy. The discovery is the first ...
Apr. 16, 2024 — A recent breakthrough study has shown potential to improve therapeutic outcomes for patients suffering from lung ...
Apr. 10, 2024 — New research sheds light on the significance of the glucocorticoid receptor in drug-resistant prostate cancer, showing that the development of drug resistance could be prevented by limiting the ...
Apr. 4, 2024 — Researchers have succeeded in correcting a gene defect that causes a hereditary liver disease and its adverse effects on ...
Mar. 21, 2024 — Researchers have discovered that a specific mutation in the cancer cells of an aggressive type of blood cancer can prevent novel immunotherapies such as CAR T-cell therapy from working. Their study ...
Mar. 6, 2024 — A specific gene may play a key role in new treatments that prevent muscle in the body from breaking down in serious muscle diseases, muscular ...
Mar. 5, 2024 — Researchers who work with tiny drug carriers known as lipid nanoparticles have developed a new type of material capable of reaching the lungs and the eyes, an important step toward genetic therapy ...
Mar. 4, 2024 — In a discovery that opens the door to a less invasive way of treating some serious disorders before birth, UC San Francisco scientists have found that delivering medicine through amniotic fluid is as ...
Feb. 23, 2024 — A new study identified a set of 140 genes that may help predict enhanced disease-free survival in patients with non-small cell lung cancer (NSCLC) treated with a combination of immunotherapy and ...
Feb. 2, 2024 — A group of patients with a hereditary disorder have had their lives transformed by a single treatment of a breakthrough gene-editing therapy, according to the lead ...
Jan. 17, 2024 — Axi-cel CAR T targets the CD19 molecule on large B-cell lymphoma cells. The ZUMA-7 trial demonstrated that axi-cel reduced the risk of disease progression, the need for new therapy, or death by 60% ...
Jan. 2, 2024 — Just like a doctor adjusts the dose of a medication to the patient's needs, the expression of therapeutic genes, those modified in a person to treat or cure a disease via gene therapy, also ...
Dec. 13, 2023 — A previously mysterious small RNA molecule in mice is found to play a crucial role in gene expression, and may be the first identified member of a new class of regulatory ...
Dec. 7, 2023 — Researchers have laid the foundation for the development of a gene therapy for the genetic heart disease arrhythmogenic cardiomyopathy (ACM). Their approach, based on replacement of the PKP2 gene, ...
Nov. 22, 2023 — Leukemia is the most common type of cancer in children. Treatment involves intensive chemotherapy, which has severe side effects due to its non-specific mode of action. A team has now discovered a ...
Nov. 16, 2023 — Researchers have discovered that 'cell competition' following gene therapy results in the accumulation of stem cells with genetic mutations which make them grow faster. Some of these ...


Comments
Post a Comment